
Designing for Health Sciences Education: Understanding Today’s Challenges
This is the first article in the six-part Designing for Health Sciences Education series.
According to the McGraw-Hill Research Foundation (pdf), “The majority of educational facilities don’t optimize learning, comfort and health but instead try to achieve top performance at the lowest cost.”1
This notable summation in a recent study is a call to action to designers of educational facilities everywhere who are seeking to create optimal learning spaces. Too often it is assumed that an aesthetically-pleasing space with plentiful light and decent acoustics is automatically conducive to learning. Or, on the opposite end of the spectrum, that space itself has no impact on learning so it’s best to settle for the cheapest option. “Can you do science in a garage?” Yes, you can, but only if you’re really motivated or driven. If the first focus of the project team is “make it look nice” or “eyes on the budget,” the learning spaces will not be the best they can be, making efficient learning and performance harder for everyone.
The first step is to ensure that the right priorities for an educational space are established. Ultimately, educational environments that become truly transformational places for learning move beyond “best practices” and integrate a deep understanding of the important themes at play within a given discipline or institution. Many factors that create excellent learning spaces do not add cost to the project if they are considered from the beginning.
When it comes to health sciences education, four intertwining themes must be understood and meaningfully incorporated to create successful learning environments for our future healthcare practitioners. These include: the acceleration of digital learning, generational influences on teachers and students, advances in understanding of how we learn, and the evolution of the field of medicine.
This series examines these themes and considers how each one can be applied to the design of health sciences education facilities and spaces. We explore the first three themes in this first article.

1.) COVID-19 and the Acceleration of Digital Learning
The COVID-19 pandemic has forced educators in all disciplines to think differently and embrace digital and technological solutions to learning. While online learning has been steadily gaining momentum across the last 15 years, the COVID-19 pandemic accelerated its widespread use, even for faculty who were otherwise reluctant to embrace it. Learning virtually is not all that different in its pure sense; it still requires that humans connect with humans. But engaging them in the online environment has its challenges. Orchestrating meaningful educational experiences that integrate both physical and virtual environments will be a key challenge of educators moving forward.
Additionally, the pandemic has fast-tracked already burgeoning healthcare delivery technologies. Moving forward into the “new normal,” it will be crucial for health sciences education to embrace training in advanced technology instrumentation, telehealth and other virtual healthcare tools. Space must reinforce this evolution in training, assuring that the proper equipment is supported and space is allocated for new types of activities.
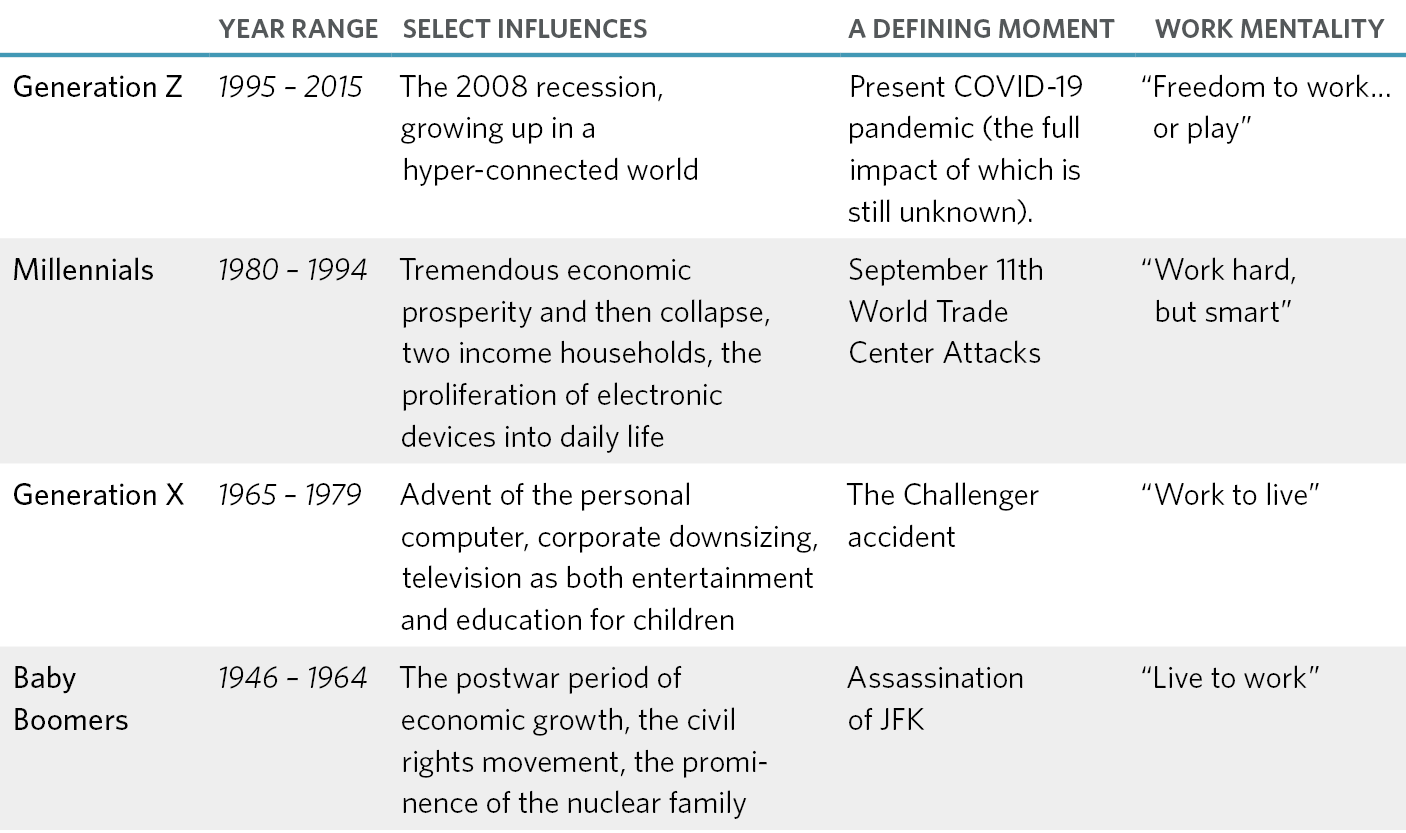
2.) Generational Influences on Students and Faculty
Today’s students and faculty come from different generations, which means they approach education with distinct and varied influences that have shaped their priorities, preferences, and expectations. Generational dynamics between students (Millennials and Gen Zers) and faculty (Baby Boomers and Gen Xers) in two areas are often at play in learning environments: technology and the motivation to learn.
Impact of Technology
Students
For Millennials and Gen Z, technology has always been part of their world and is considered a matter of course. The average Gen Zer received their first smartphone at the age of 10.3 years, and spends an average of three hours a day on their phone (for many purposes including learning, texting and, to a lesser extent, talking). Both generations move seamlessly between multiple devices.
Faculty
Baby Boomers and Gen Xers, on the other hand, are quite different in their respective characteristics; both experienced the development and adoption of technology in a much more linear fashion than did today’s students. Neither Baby Boomers nor Gen Xers are considered “digital natives,” so they tend to focus on one thing at a time and check off their to-dos in an organized fashion. For them, moving back and forth between multiple devices seems counterproductive.
Since it’s human nature to try to repeat (or recreate) previously successful experiences, faculty members may cling to the idea that devices are a distraction, that multitasking is impossible, and that they need to lecture and deliver content in a linear fashion. And while these four generations can learn new things from each other, it’s critical to adapt teaching methodologies to the typical patterns and work habit of students — and not the other way around.
The future will demand technology-rich, multi-modal learning experiences and faculty must be nimble enough to continue to learn as new technologies emerge in both education and healthcare. In order to accomplish this, educational institutions will need to have space that facilitates faculty training – and facilities personnel must consider how the design of classrooms, instructional laboratories and simulation experiences can allow an instructor to seamlessly teach students in situ and remotely at the same time and provide meaningful connections.
Motivation to Work and Learn
Since Gen Zers are always connected, the lines between school or work and home are blurred. They are competitive, want to be judged on their own merit, and prefer to study and work independently. But they also prefer their communication with others to be face-to-face rather than online. Both Millennials and Gen Zers are willing to work hard, but they also need to understand the point of the task. This contrasts with Baby Boomers and Gen Xers, who were trained to work hard on assigned tasks without necessarily questioning why and so may not be motivated by the same factors.
The result is a disconnect between how faculty were educated and how they can best educate. Today’s students have little interest in memorizing material and prefer to manage information. Consequently, if they aren’t motivated or understand the point of the work, the environment might present additional obstacles to learning. That means educational tasks for students today must be both engaging and relevant, and the space where this education takes place must support this goal.
3.) Advances in Understanding How We Learn
While generational distinctions need to be considered in the design of health education space, we must also consider other discoveries made in the last 30 years about how people learn.
Human Development & Training for Decision-Making
We know now that the brain is not fully formed until the mid- to late-twenties.7 Today’s youngest nursing students may have entered university and/or nursing school directly after high school, while even the youngest medical students already have an undergraduate degree when they begin medical school (although this model may be changing). While both groups of students are in the health sciences, their ages, and therefore stage of brain development, may be quite different.
The trend toward interprofessional education in the academic health center supports training students in the technical aspects of their professions, as well as how to form the best judgments and make the best decisions. This decision-making process is as much a biological process as a cognitive one. In the IPE model, some students may be 10 years ahead of others in the physical formation of their brains. In order to challenge them equally, we must be ready for different perceptions and input.
However, many 20th-century facilities and traditional teaching approaches were not developed with this understanding of the physiology of the brain. For example, one of the hallmarks in any medical or nursing educational institution is the famous “lecture hall.” These were typically designed to accommodate one cohort, and at many institutions there are four nearly identical lecture halls, one for each year of medical school. These large rooms are typically tiered, with theater-style seating and a small pull-up tablet to accommodate a (paper) notebook for students to write notes, frantically copying information from the screen while trying to comprehend the verbal lesson. These older lecture halls may not have originally accommodated wheelchairs, and while many have been retrofitted to do so, these spaces are often at the top or the bottom, precluding their owners from sitting with friends wherever they like. During the lecture, students were generally presented with initial concepts, expected to study them, and then show up to various clinical skills locations to master these concepts in hands-on but separate activities and spaces.
The problem, however, is that this isn’t how people actually learn … at least, not optimally. The transformative book "How People Learn," originally published in 1990 and updated in 2017, contained revolutionary findings about how the brain works and how people actually process new information.8 For a more thorough discussion of these early findings, see Designing for How We Learn: How We Got Here.
If we put the learner first by identifying effective communication with learners as our primary goal, our view of what comprises good learning environments naturally changes.
The Truth about Attention
It’s well-documented that the human attention span, regardless of a person’s age or IQ, ranges between 10 and 17 minutes of close attention to a single thing or idea. The dedicated teacher takes advantage of that knowledge to switch gears during a class period — to move from one topic to another, to move from lecture to small group discussion, or to allow their students to refocus in many other ways.
With this greater understanding of how people learn, health sciences schools must look to transition their teaching facilities away from the industrial age to learning environments that reflect our digital lifestyle. Progressive institutions are beginning to evaluate space based on its effectiveness rather than solely on the cost of renovating it. Those large, steeply tiered lecture halls, with tiny tablet arms for taking handwritten notes, often sit in the most valuable real estate within a medical school and yet are the least effective learning spaces. It may be time to embrace a big-picture perspective of the kinds of space that a health sciences education institution needs in its portfolio and identify a strategy for getting there.

4.) Evolution of Medicine
In addition to the factors above, the evolution of medicine and its impact on healthcare delivery has extraordinarily influenced the types of spaces and environments required for health science education. Interprofessional education, precision medicine and a shift toward “well care” and population health are among the most significant impacts on healthcare, and by association on health science education, today. In our next article, we’ll look at these trends and their potential impacts on the learning environments of health professions students.
References
- Baker, Lindsay, and Harvey Bernstein. McGraw-Hill Research Foundation and the Center for Green Schools, 2018, The Impact of School Buildings on Student Health and Performance (pdf).
- Seemiller, Corey, and Meghan Grace. Jossey Bass, A Wiley Brand, 2016, Generation Z Goes to College.
- Purdue University. “Generational Differences in the Workplace [Infographic].” Purdue Global, 2009.
- “3 No-Nonsense Tips for Effectively Managing Gen Z.” Insperity, 13 July 2017, Accessed 21 May 2021.
- Jenkins, Ryan. “How ‘Lazy’ Millennials Are Transforming Hard Work.” Inc.com, 3 Feb. 2016, Accessed 21 May 2021.
- Rampton, John. “Different Motivations for Different Generations of Workers: Boomers, Gen X, Millennials, and Gen Z”, 17 Oct. 2017
- “Lifespan Development.” Lumen Learning, Lumen, courses.
- Washington, D.C. National Academies Press, 2018, How People Learn II: Learners, Contexts and Cultures.
